Overview
 Also known as Morton’s Interdigital Neuroma, Morton’s Metatarsalgia, Morton’s Neuralgia, Plantar Neuroma, Intermetatarsal Neuroma) What is a Morton’s neuroma? Morton’s neuroma is a condition characterized by localized swelling of the nerve and soft tissue located between two of the long bones of the foot (metatarsals – figure 1), which can result in pain, pins and needles, or numbness in the forefoot or toes.
Also known as Morton’s Interdigital Neuroma, Morton’s Metatarsalgia, Morton’s Neuralgia, Plantar Neuroma, Intermetatarsal Neuroma) What is a Morton’s neuroma? Morton’s neuroma is a condition characterized by localized swelling of the nerve and soft tissue located between two of the long bones of the foot (metatarsals – figure 1), which can result in pain, pins and needles, or numbness in the forefoot or toes.
Causes
When a nerve is pinched between bones, the result is swelling of the nerve. It is this swelling which is referred to as a Neuroma. When the condition occurs in the foot, it is known as a Morton?s Neuroma. Morton?s Neuroma is technically not a tumor. Rather, it is a thickening of the tissue that surrounds the digital nerves leading to the toes. These nerves allow for physical sensation on the skin of the toes. The region of inflammation is found where the digital nerve passes under the ligament connecting the toe bones (metatarsals) in the forefoot. Morton?s Neuroma commonly develops between the third and fourth toes, generally as a result of ongoing irritation, trauma or excessive pressure. In some cases, the second and third toes are involved. Morton?s Neuroma is confined to one foot in most cases, though it can occur in both, particularly in athletes such as runners.
Symptoms
Symptoms associated with a neuroma include a dull burning sensation radiating towards the toes, a cramping feeling, or even a stinging, tingling sensation that can be described as being similar to an electric shock. It is often worse when wearing shoes with most people finding the pain disappears when removing their shoes.
Diagnosis
Your podiatric physician will begin by taking a history of your problem. Assist him or her by describing your condition as well as you can. Keep track of when the symptoms started and how, any changes you?ve noted (whether the pain has gotten worse, or whether other symptoms have appeared as well, etc.). If you?ve noticed that certain activities or footwear make things worse or bring about additional symptoms, be sure to mention that. If you work in specific footwear, or if you participate in any certain sports, bring the shoes you use. Your doctor may be able to learn quite a lot about your condition that way!
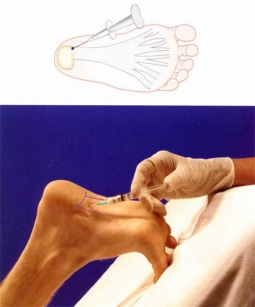
Non Surgical Treatment
Initial therapies are nonsurgical and can involve one or more of the following treatments Changes in footwear. Avoid high heels or tight shoes, and wear wider shoes with lower heels and a soft sole. This enables the bones to spread out and may reduce pressure on the nerve, giving it time to heal. Custom shoe inserts and pads also help relieve irritation by lifting and separating the bones, reducing the pressure on the nerve. One or more injections of a corticosteroid medication can reduce the swelling and inflammation of the nerve, bringing some relief. Massaging the affected area can provide some momentary relief. Several studies have shown that a combination of roomier, more comfortable shoes, nonsteroidal anti-inflammatory medication, custom foot orthoses and cortisone injections provide relief in over 80 percent of people with Morton?s Neuroma. If conservative treatment does not relieve your symptoms, your physician may discuss surgical treatment options with you.
Surgical Treatment
Surgery to excise the neuroma is usually performed under general anaesthetic in a day surgery facility. After surgery you will have to keep your foot dry for two weeks. Generally neuroma surgery allows for early weight bearing and protection in some type of post op shoe gear. Some neuromas may reoccur, but this is rare. Most studies on patient satisfaction after neuroma surgery show approximately 90% reduction of pain and about 85% of all patients rated the overall satisfaction with the results as excellent or good.
 Overview
Overview Symptoms
Symptoms Prevention
Prevention





 Achilles tendonitis is one of the most common running injuries. The achilles tendon is the large tendon at the back of the ankle. It connects the calf muscles made up of the gastrocnemius and soleus to the heel bone or calcaneus. It provides the power in the push off phase of walking and running where huge forces are transmitted through the achilles tendon. Achilles tendonitis is often now referred to as achilles tendinopathy. This is because the term tendinopathy covers all types of overuse achilles tendon injury. Strictly speaking tendonitis suggests an inflammatory condition of the tendon but in reality few achilles tendon injuries are actually down to pure inflammation. Soleus muscleThe main finding, particularly in older athletes is usually degeneration of the tissue with a loss of normal fibre structure. Other very similar conditions may actually be due to inflammation or degeneration of the tendon sheath which surrounds the tendon rather than the achilles tendon itself. In addition to being either chronic or acute, achilles tendonitis can also be at the attachment point to the heel called insertional achilles tendonitis or in the mid-portion of the tendon typically around 4cm above the heel. Healing of the achilles tendon is often slow, due to its poor blood supply.
Achilles tendonitis is one of the most common running injuries. The achilles tendon is the large tendon at the back of the ankle. It connects the calf muscles made up of the gastrocnemius and soleus to the heel bone or calcaneus. It provides the power in the push off phase of walking and running where huge forces are transmitted through the achilles tendon. Achilles tendonitis is often now referred to as achilles tendinopathy. This is because the term tendinopathy covers all types of overuse achilles tendon injury. Strictly speaking tendonitis suggests an inflammatory condition of the tendon but in reality few achilles tendon injuries are actually down to pure inflammation. Soleus muscleThe main finding, particularly in older athletes is usually degeneration of the tissue with a loss of normal fibre structure. Other very similar conditions may actually be due to inflammation or degeneration of the tendon sheath which surrounds the tendon rather than the achilles tendon itself. In addition to being either chronic or acute, achilles tendonitis can also be at the attachment point to the heel called insertional achilles tendonitis or in the mid-portion of the tendon typically around 4cm above the heel. Healing of the achilles tendon is often slow, due to its poor blood supply.





You must be logged in to post a comment.